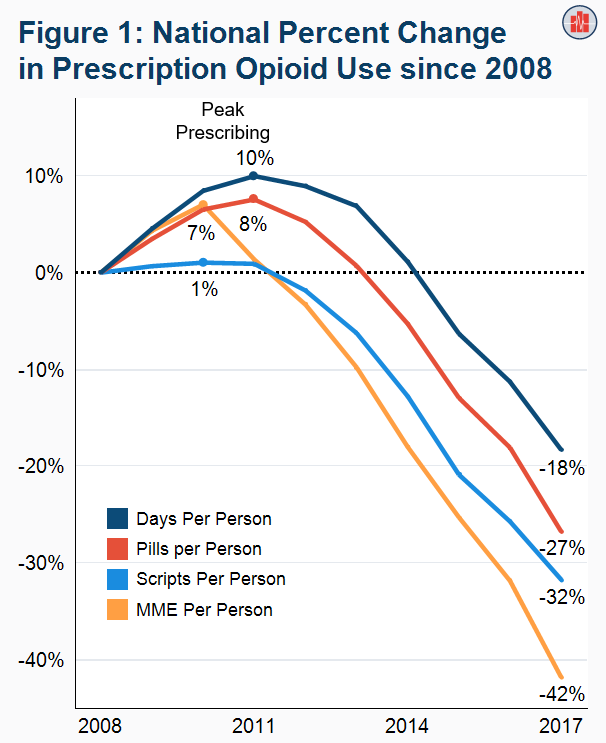
A medication needn't be banned, only shamed sufficiently to have profound effects. Case in point: prescription opiates, which only about 7% of people become hooked on, which also tracks slightly higher than the 5% of people who become alcoholics. Take a look at opiate prescriptions between 2008 and 2017 here:
A medication needn't be banned, only shamed sufficiently to have profound effects. Case in point: prescription opiates, which only about 7% of people become hooked on, which also tracks slightly higher than the 5% of people who become alcoholics. Take a look at opiate prescriptions between 2008 and 2017 here:
Doctors stopped prescribing opioids because of so much media noise about the "opioid crisis" and what happened next was all-too predictable—take a look at fentanyl overdoses.
This is really interesting, but it's hard to draw a causal link here. Opioid prescriptions were rising during the same period fentanyl overdoses were flat. And overdoses didn't start to spike until 2015, long after opioid prescriptions were way down. I'm not saying there can't be a causal relationship there, but it's not clear.
That said, yes, addiction and abuse of other, more dangerous drugs are among the risks and long-term implications I'm talking about. I think it's absolutely right that there was a conversation about opioid addiction. Don't you? 7% isn't nothing. But I also think it should be framed in a way that makes it clear that in most cases, opioids aren't addictive. Basically, I'm advocating a clear eyed analysis of the costs and benefits. That's not happening with puberty blockers.
"This is really interesting, but it's hard to draw a causal link here. Opioid prescriptions were rising during the same period fentanyl overdoses were flat. And overdoses didn't start to spike until 2015, long after opioid prescriptions were way down. I'm not saying there can't be a causal relationship there, but it's not clear."
Sure, but that's true of literally everything epidemiological (which cannot establish causation)—including any discussion about puberty blockers.
"I think it's absolutely right that there was a conversation about opioid addiction. Don't you?"
I think it would've been had it been had honestly. But it was not. Which makes me wonder if we're capable of honest dialogue any longer in our (social) media ecosystem. The only reason I know all this is because it's my own upcoming article (I've researched for a year).
The thing is, almost no one is saying, "Yes, opiates are addictive, but there's only a 7% chance you'll become hooked."
7% isn't nothing, you're right, but it's just like (and often less than) any other side effect of any other drug, side effects that are usually minuscule-print footnotes.
So why the glaring discrepancy?
We don't have a "vaccine side effect crisis," a "peanut butter allergy crisis," or a "this psoriasis drug can cause you to poop water and drop-dead *crisis*" because a small number of people experience negative effects. We don't attach *crisis* to any other side effect except addiction, including ones that kill people.
190,000 people died from OxyContin between 1999 and 2017. Sounds scary and all, but 643,826 people died from car accidents during the same period, dwarfing OxyContin deaths. Do we have a driving *crisis* now?
"I'm advocating a clear-eyed analysis of the costs and benefits. That's not happening with puberty blockers."
I'm all for a clear-eyed analysis of the costs and benefits. I also realize it's not my business if people want to take them despite (reasonable) risks identified. The same principle as above applies here.


{kind=link}
A medication needn't be banned, only shamed sufficiently to have profound effects. Case in point: prescription opiates, which only about 7% of people become hooked on, which also tracks slightly higher than the 5% of people who become alcoholics. Take a look at opiate prescriptions between 2008 and 2017 here:
https://healthcostinstitute.org/images/easyblog_articles/314/b2ap3_large_Figure-1-Change-in-Us_20190715-165510_1.png
Doctors stopped prescribing opioids because of so much media noise about the "opioid crisis" and what happened next was all-too predictable—take a look at fentanyl overdoses.
https://ca-times.brightspotcdn.com/dims4/default/e9b14ea/2147483647/strip/true/crop/1280x720+0+0/resize/840x473!/quality/90/?url=https:%2F%2Fcalifornia-times-brightspot.s3.amazonaws.com%2F32%2Fd0%2Fd879cb32d373e82e04cfaccaa86c%2Fla-1553140571-pob09qlwxw-snap-image
No bans need apply.
This is really interesting, but it's hard to draw a causal link here. Opioid prescriptions were rising during the same period fentanyl overdoses were flat. And overdoses didn't start to spike until 2015, long after opioid prescriptions were way down. I'm not saying there can't be a causal relationship there, but it's not clear.
That said, yes, addiction and abuse of other, more dangerous drugs are among the risks and long-term implications I'm talking about. I think it's absolutely right that there was a conversation about opioid addiction. Don't you? 7% isn't nothing. But I also think it should be framed in a way that makes it clear that in most cases, opioids aren't addictive. Basically, I'm advocating a clear eyed analysis of the costs and benefits. That's not happening with puberty blockers.
"This is really interesting, but it's hard to draw a causal link here. Opioid prescriptions were rising during the same period fentanyl overdoses were flat. And overdoses didn't start to spike until 2015, long after opioid prescriptions were way down. I'm not saying there can't be a causal relationship there, but it's not clear."
Sure, but that's true of literally everything epidemiological (which cannot establish causation)—including any discussion about puberty blockers.
"I think it's absolutely right that there was a conversation about opioid addiction. Don't you?"
I think it would've been had it been had honestly. But it was not. Which makes me wonder if we're capable of honest dialogue any longer in our (social) media ecosystem. The only reason I know all this is because it's my own upcoming article (I've researched for a year).
The thing is, almost no one is saying, "Yes, opiates are addictive, but there's only a 7% chance you'll become hooked."
7% isn't nothing, you're right, but it's just like (and often less than) any other side effect of any other drug, side effects that are usually minuscule-print footnotes.
So why the glaring discrepancy?
We don't have a "vaccine side effect crisis," a "peanut butter allergy crisis," or a "this psoriasis drug can cause you to poop water and drop-dead *crisis*" because a small number of people experience negative effects. We don't attach *crisis* to any other side effect except addiction, including ones that kill people.
190,000 people died from OxyContin between 1999 and 2017. Sounds scary and all, but 643,826 people died from car accidents during the same period, dwarfing OxyContin deaths. Do we have a driving *crisis* now?
"I'm advocating a clear-eyed analysis of the costs and benefits. That's not happening with puberty blockers."
I'm all for a clear-eyed analysis of the costs and benefits. I also realize it's not my business if people want to take them despite (reasonable) risks identified. The same principle as above applies here.